The beginnings of autism as a clinical diagnosis
During the 1930's, child psychiatrist Leo Kanner started to notice in some children referred to his Baltimore clinic a cluster of characteristics that were not described by any of the existing diagnoses he had at his disposal. Donald Triplett, the first person to be diagnosed as autistic, was one of these children. Kanner noted that Donald was 'happiest when left alone, almost never cried to go with his mother... wandered about smiling, making stereotyped movements with his fingers...[and] spun with great pleasure anything he could seize upon to spin'. Kanner also observed that 'words to [Donald] had a specifically literal, inflexible meaning' and that when Donald entered a new room, 'he completely disregarded the people and instantly went for objects' (Kanner, 1943).
Based on his observations of Donald and of ten other children, Kanner (1943) inferred the existence of a clinical syndrome which was, in his view, fundamentally characterised by 'an inability to relate... in the ordinary way to people and situations from the beginning of life'. Accordingly, he named this new entity 'autism', a term borrowed from the schizophrenia literature to describe a state of detachment from the outside world. Kanner also noted in the children at his clinic a second cardinal feature of autism: 'an obsessive desire for the maintenance of sameness', which drove a tendency towards repetition and ritual, along with a marked aversion to change. He concluded that, whilst most of the cases he described had been previously considered to be 'feebleminded' (i.e., in today's terms, to have an intellectual disability), they were, in fact, 'all unquestionably endowed with good cognitive potentialities'.
Around the same time as Kanner was making his observations of 'autistic disturbances of affective contact', several other clinicians in different countries were formulating and reporting a similar entity. These included Hans Asperger (1944) in Vienna, Mildred Creak (1937) in London, and, earliest of all, Grunya Efimovna Sukhareva (1926) in Moscow. Kanner did not acknowledge any of this work in his original autism paper, professing to describe a condition that differed 'from anything reported so far'. It has become a matter of debate amongst historians about how the work of Asperger and his colleagues and of Sukharvena may have shaped Kanner's formulation of autism, including consideration of whether Kanner deliberately understated these influences (Silberman, 2015). Nevertheless, it was Kanner's work (published in English) that introduced autism to mainstream nosology in the USA, UK, and beyond, with the contributions of others remaining relatively obscure until their rediscovery after autism was already an established diagnosis.
There is substantial continuity between Kanner's original description of autism and how the condition is understood today, 80 years later. Autism continues to be conceptualised at the behavioural level, as a collection of observable behaviours and reportable experiences: there is still no biomarker for autism, despite decades of research directed towards discovering its neurobiological essence. As such, in common with almost all conditions in psychiatry, autism is diagnosed via observation of its manifestations (i.e., its 'symptoms'); and the manifestations proposed by Kanner have much in common with those used in contemporary practice. In line with Kanner's initial account, the Diagnostic and Statistical Manual of Mental Disorders, 5^th^ Edition (DSM-5; Association, 2013) and the International Classification of Diseases, 11^th^ Revision (ICD-11; World Health Organisation, 2019), which govern diagnostic practice, define autism as having two types of symptom, the first concerning difficulties with social relating and social communication; and the second encompassing a range of repetitive behaviours reflecting a powerful desire for sameness.
Changes in how autism is understood
Nevertheless, in the context of a stable consensus about autism's core features, there have been substantial shifts in how the condition is understood. In this section, I highlight four key changes to the conceptualisation of autism in the years since Kanner's initial, foundational formulation.
From category to dimension
First, whereas autism was once considered a categorical disorder, it is now widely understood to be dimensional. The original, categorical conceptualisation of autism held it to be a qualitatively distinct developmental outcome, fundamentally different from both typical development and from other conditions, such as intellectual disability or attention deficit/hyperactivity disorder. From the 1970s onwards, theoretical and clinical work, in particular by the British psychiatrist Lorna Wing, challenged this view, proposing instead that autism is better understood as being at one end of a continuous trait distribution that extends through the population, with no natural cut point between autistic and non-autistic people (see Figure 1).
Figure 1 Autism as a dimensional condition
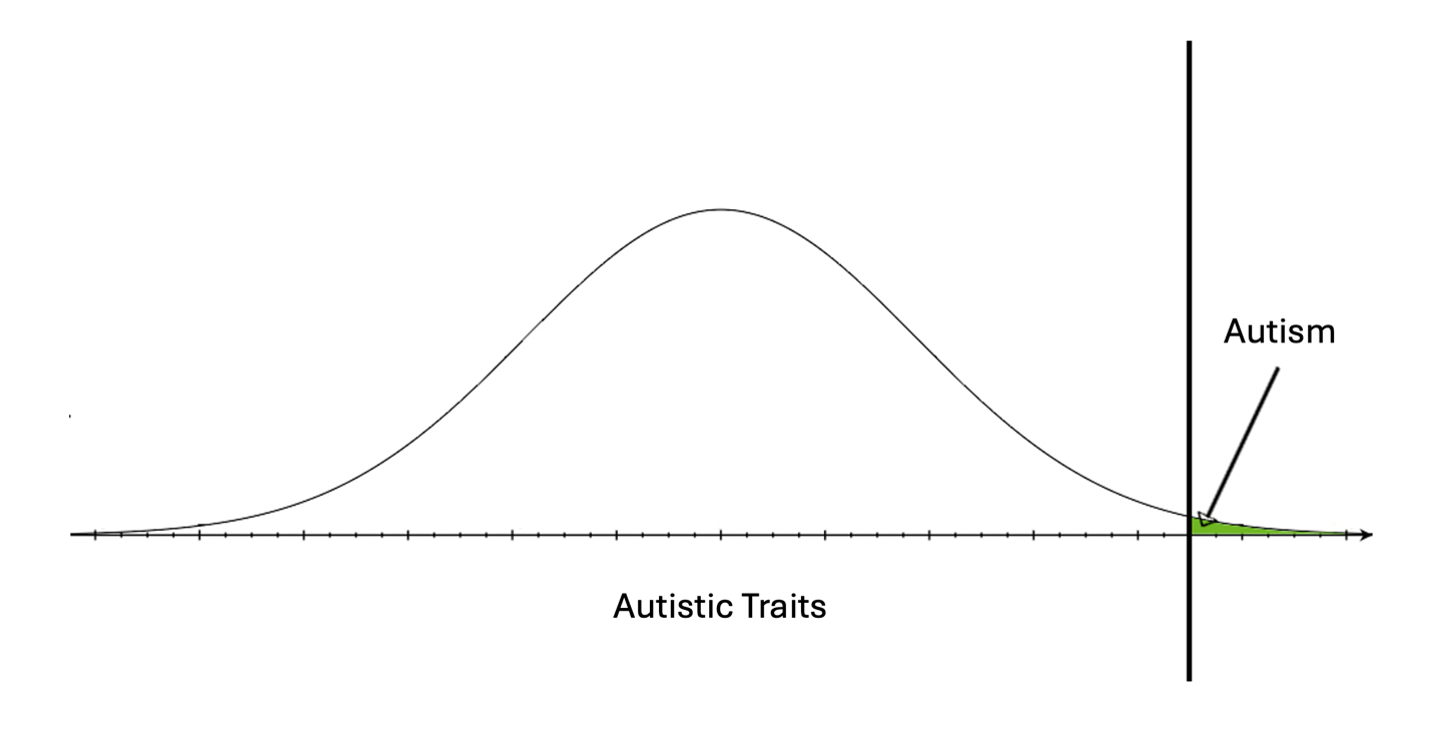
Empirical work is supportive of the dimensional conceptualisation of autism. Research on the family members of autistic people discovered that relatives often have autistic characteristics, labelled 'a broader autism phenotype', without meeting full diagnostic criteria (Piven et al., 1997). Subsequently, studies of sub-diagnostic autistic characteristics in whole-population samples revealed that such autistic traits are not limited to the relatives of autistic people but, rather, are common in the general population. These are continuously distributed, with no 'zone of rarity' between individuals with an autism diagnosis and those who have high autistic traits, but are not, by convention, autistic (Constantino & Todd, 2003; Skuse et al., 2004). As such, the threshold for diagnosis - the line that imposes on a continuum the binary distinction of 'autistic' and 'not autistic' - is arbitrary and negotiable.
The causes of autism
A second fundamental shift is in the understanding of what causes a person to be autistic. Kanner's original account of autism emphasised its presence from the very beginning of life, which led him to downplay the possibility that environmental factors (such as quality of parenting) played an important part in the aetiology of autism (Kanner, 1943). However, partly reflecting the hegemony of psychoanalysis in American psychiatry at the time, Kanner and others came to hold and propagate psychogenic explanations of autism (Eisenberger & Kanner, 1956). Most influentially, Bruno Bettelheim (1967) popularised the idea that a cold, undemonstrative, and rigid style of parenting caused autism, with a particular focus on blaming mothers. This unfortunate idea came to be known as the 'refrigerator mother hypothesis'.
Subsequent quantitative and molecular genetic research has disproven the proposal that autism is caused by parenting. The first twin study of autism revealed it to have a high heritability (Folstein & Rutter, 1977), and this has since been replicated multiple times (Tick et al., 2016). Autism is amongst the most heritable of all the conditions in psychiatry and psychology. Autistic traits across the full spectrum of intensity are also highly heritable (Ronald & Hoekstra, 2011); with evidence for shared genetic effects on a person's level of autistic traits and on their probability of meeting criteria for autism, as would be expected for a dimensional condition (Robinson et al., 2011).
The neurodiversity paradigm
A third key development is in the understanding of how the disability and distress commonly experienced by autistic people arise. This has been characterised as a paradigm shift from a 'pathology model' to a 'neurodiversity model' (Pellicano & den Houting, 2021), representing a reinterpretation of empirical data, effected by the growing influence of autistic thinkers on autism research and practice (Botha et al., 2024).
For most of its history, autism has been widely viewed as a form of psychopathology, uncritically assumed to be a disorder that is a collection of impairments which directly and inevitably give rise to disability. By contrast, the neurodiversity model reframes autism as a form of difference, often referred to as 'neurodivergence' (Pellicano & den Houting, 2021). Within this framework, the disability and distress so commonly experienced by autistic people are understood, not as an inevitable consequence of neurodivergence, but rather as arising from a misfit between the individual and their environment (Chapman & Botha, 2023). As such, the neurodiversity paradigm is the expression of a tradition that includes the social model of disability (Oliver, 1990) and developmental psychopathology (Cicchetti & Cohen, 1995), which characterise adaptation and maladaptation as arising from a dynamic interaction, over time, between the person and their context (Mandy & Lai, 2016).
The neurodiversity paradigm draws on the understanding that autistic people commonly live in physical and social environments made by and for non-autistic people; and that these are commonly challenging, unaccommodating, and/or hostile to their autistic inhabitants. This helps explain why autistic people who share similar levels of autistic characteristics and intelligence can experience such diverse outcomes; why individual characteristics of autistic people are poor predictors of functioning and wellbeing; and why key life stage transitions, when the environment but not the individual undergoes a rapid and substantial change, often cause major shifts in disability and distress (Howlin & Magiati, 2017).
The neurodiversity paradigm has important implications for supporting autistic people. Historically, efforts at enhancing the lives of autistic people, informed by the pathology model, have commonly focused on changing the autistic person to reduce their impairments and thereby reduce disability. By contrast, a neurodiversity approach seeks to address person-environment fit, which often involves interventions to model the environment to make it more accommodating (Chapman & Botha, 2023).
The changing prevalence of autism
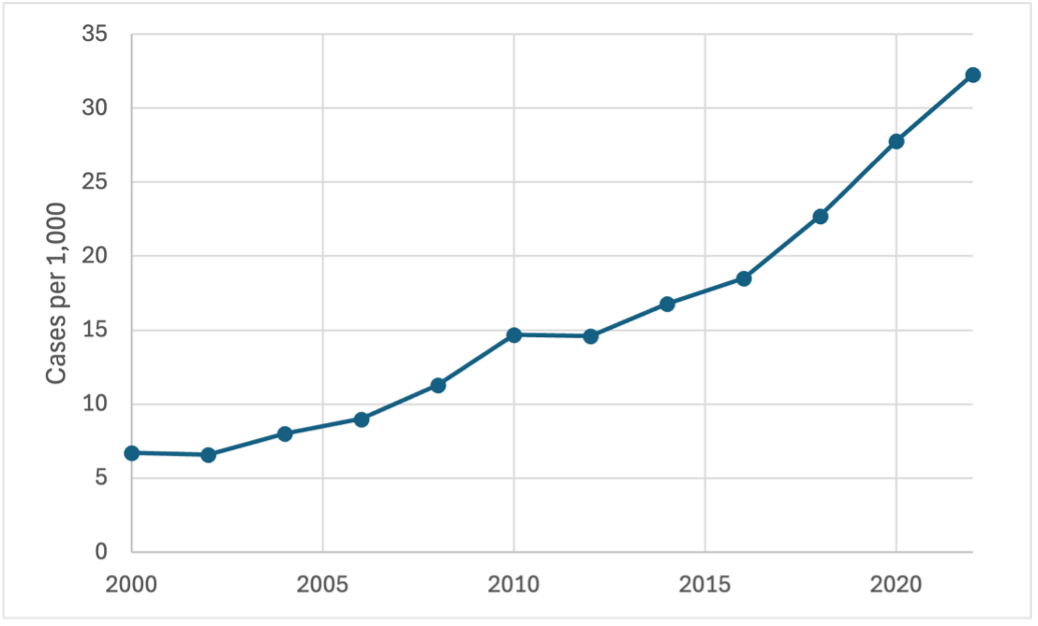
The fourth change relates to understandings of how common autism is. Throughout his career, Kanner insisted that autism was a rare condition, and when the first autism epidemiological prevalence study was conducted in the 1960s, its findings supported his view. This research screened a whole population of eight to 10-year-olds in the county of Middlesex in England, identifying just 35 autistic children, which suggested that around 1 in 2,500 were autistic (Lotter, 1966). Up until the end of the 1990s, prevalence studies of autism tended to confirm the view that autism was rare. But from then onwards began a phenomenon that has continued to this day: the growth of autism's estimated prevalence. A striking example is provided by research from the US Centres for Disease Control (Figure 2). Their estimates of autism's prevalence have gone up nearly five-fold since 2000, with the most recent figures suggesting that one in 31 American children is autistic (Shaw et al., 2025). A similar pattern can be observed in the UK, where one study of health records up to 2018 found that 1 in 35 14 to 19-year-olds have an autism diagnosis (O’Nions et al., 2023). Compared to Lotter's original prevalence estimates in the mid 1960s, that represents an approximate 70-fold increase.
Figure 2 Estimated autism prevalence in the USA from successive studies by the Centres for Disease Control (CDC)
High and increasing rates of autism diagnosis since the late 1990s are not universal. The phenomenon is most pronounced in high-income countries, and there is substantial variability in diagnostic rates within these nations (Global Burden of Disease Study 2021 Autism Spectrum Collaborators, 2025). Whilst anglophone nations, such as the USA, UK, Canada and Australia are especially likely to have high diagnostic rates, there are also high levels of autism diagnosis in other high-income countries, for example, Japan, the Netherlands, and South Korea.
Another notable feature of the trend towards ever-higher rates of autism diagnosis concerns the distinction between epidemiological prevalence and administrative prevalence. Epidemiological prevalence is the rate of autism in a population, as estimated by studies that screen a defined population and seek to identify cases according to standardised assessment protocols, regardless of whether or not they already have a clinical diagnosis. Administrative prevalence is the proportion of the population who have received an autism diagnosis. In some wealthy, industrialised nations, the rates of administrative prevalence now exceed rates of epidemiological prevalence. For example, in the UK, the most recent epidemiological prevalence estimate for autism in children is 1.16% (Baird et al., 2006), whereas administrative prevalence rates are around 3% (O’Nions et al., 2023). Similarly, in the USA, administrative prevalence substantially exceeds epidemiological prevalence estimates (Shaw et al., 2025).
Why are rates of autism diagnosis rising?
The growth in autism diagnosis described above is a complex, multidetermined phenomenon (Charman, 2025; Brede et al., 2022; Zeidan et al., 2022). Given the regional variations highlighted above, it is likely that in each country where it has occurred, it is shaped by a unique combination of factors. In this section, I outline three key ideas that have been proposed to drive the growth of autism diagnosis. My focus is mainly on wealthy, anglophone countries, in particular the USA and UK. This reflects the fact that the growth of autism diagnosis has been especially striking in those nations, and that most empirical evidence relevant to understanding the phenomenon originates from these countries.
An autism epidemic?
One potential explanation for the growth in diagnoses is that autism has simply become more common. Given the precipitous rise in diagnostic rates described above, this has led some to believe that there is an 'autism epidemic'. This idea has been prominent in public discourses about autism since the 1990s and has, recently, become influential on policy in the USA; but it lacks validity. As discussed above, an individual's chances of being autistic and/or of having high autistic traits are strongly influenced by genetic variability. It is implausible that very substantial increases in rates of diagnosis over only a few decades could be caused by the neurobiological entity of autism becoming more common, given that this would require a rapid and dramatic change in the genetic composition of the population.
Because genetic accounts of the aetiology of autism are incompatible with the existence of an autism epidemic, its proponents require theories about the introduction of new environmental factors that cause autism. This has included proposals that pollution, pain killers taken in pregnancy, screen time, and vaccines cause autism, thereby driving the growth in diagnosis. Such claims tend to be based on unsound interpretations of data. Perhaps the most notorious proposal of this type has been that vaccines cause autism, which started to become prominent in public discourses about rising autism rates in the 1990s, in part due to its adoption by influential parent-activists (Silberman, 2015). This likely reflects the fact that some vaccines are given in infancy and early childhood, around the time that autistic characteristics become apparent in some children, and at an age when a subgroup of children experience a developmental stasis or regression (Tan et al., 2021).
Belief that vaccines were causing an autism epidemic was stoked by a paper published in one of the world's leading medical journals by Dr Andrew Wakefield and colleagues, that appeared to suggest a link between administration of the MMR vaccine and the development of autism, mediated by gastro-intestinal difficulties (Wakefield et al., 1998). The paper has since been retracted, due to the discovery of significant methodological flaws, data manipulation and undeclared conflicts of interest. A large body of subsequent research has shown no link between vaccines (including the MMR) and autism (Taylor et al., 2014). Despite this, anxieties about the possible role of vaccines in causing autism are still widespread, with resultant negative consequences for public health, due to their effects on uptake of vaccination programmes.
An epidemic of discovery?
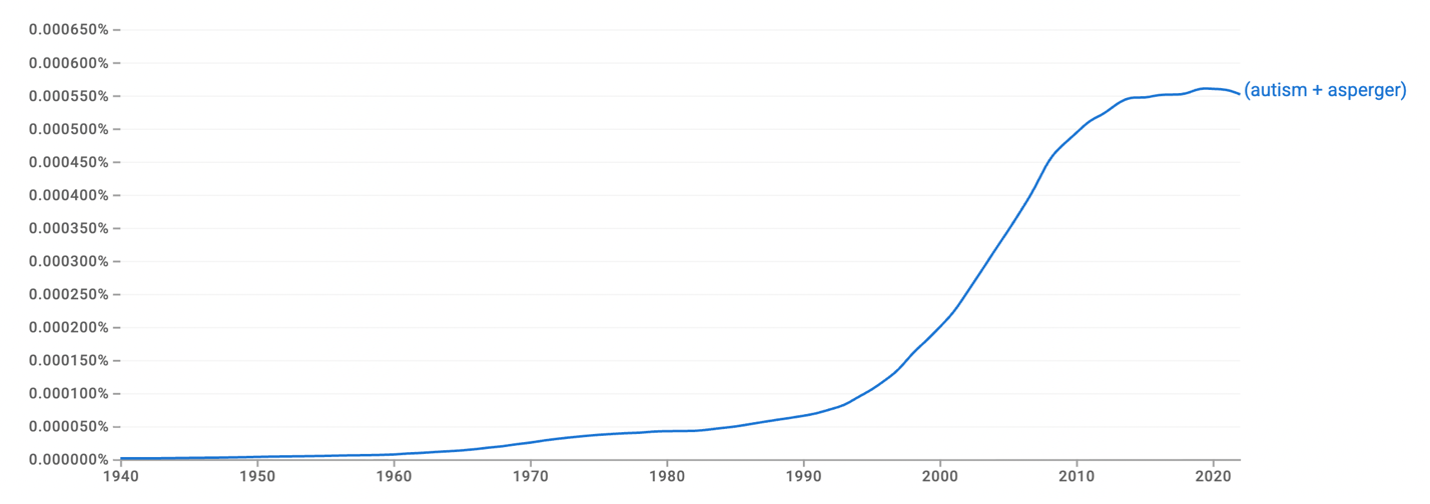
Given the lack of evidence for an increase in the neurobiological entity of autism as an explanation for the marked growth in diagnoses since the 1990s, some have proposed that there may be, rather than an autism epidemic, an epidemic of discovery. This is a highly plausible idea, since there have been several changes during the period in question that would give rise to improved identification of autism. First, public awareness of and interest in autism has grown substantially since the 1990s. This is consistent with Figure 3, which used Google Ngram to chart the use of the words 'autism' and 'Asperger' in a corpus of books between 1940 and 2022. There is a notable point of inflection during the 1990s. Second, an increase in knowledge has likely corresponded with a decrease in stigma against autistic people in many countries (Sasson & Morrison, 2019). Third, during the time in question, improved assessment measures and protocols have been developed and disseminated. Fourth, services in many countries, including the USA and UK, have greatly expanded, improving access to assessment.
Consideration of diagnostic rates amongst adults offers further evidence that there have been improvements in the recognition of autism since the 1990s. Even in countries such as the UK, where diagnostic rates for children and adolescents are high, autism is substantially underdiagnosed amongst those who reached adulthood before the late 1990s. O'Nions and colleagues (2023) found that of those aged 40 to 49 years in 2018, only .3% had an autism diagnosis on their primary care health records, which is substantially below even conservative estimates of the epidemiological prevalence of autism in UK adults (Brugha et al., 2016). Adult autism clinics report assessing numerous individuals who have reached adulthood without an autism diagnosis, despite clearly meeting full criteria for the condition and having longstanding autistic characteristics and associated disability since early childhood (Ashwood et al., 2016).
Figure 3 Use of the words 'autism' and 'Asperger' since 1940 (Derived from Google NGram Viewer)
A broadening of the diagnostic category
Whilst improvements in recognition of autism have contributed to rising diagnostic rates, this does not account for the totality of the increase. Consideration should also be given to another key change: a broadening of the diagnostic construct of autism.
On the 13^th^ of November 2017, the American Heart Association (AHA) announced that they were changing the threshold for diagnosing hypertension, lowering it from 140/90 mmHg to 130/80 mmHg. The decision was based on data that showed a 10 mmHg reduction in blood pressure lowers a person's chance of cardiovascular problems and reduces all-cause mortality by 13%. In consequence of the AHA's change, overnight an extra 30 million Americans were classified as having high blood pressure: of course, this was not because their blood pressure had risen; rather, they found themselves within the boundaries of a newly broadened definition of hypertension.
Something analogous to the AHA's broadening of the definition of hypertension has happened with autism. This is most clearly shown by consideration of changes to diagnostic criteria for autism as set out in the diagnostic manuals that govern clinical practice. Autism entered the Diagnostic and Statistical Manual (DSM) in its third edition, in 1980 (APA, 1980). Named 'infantile autism' in DSM-III, it was presented as per Kanner's original conception of a rare, categorical, and severe disorder. Individual symptoms were described in stark terms, as 'gross deficits' and 'bizarre responses', and they only counted towards a diagnosis if they had appeared prior to 30 months. Further, in DSM-III, autism was defined as a monothetic condition: to qualify for a diagnosis, an individual had to show evidence of every one of the criteria. Only a fraction of the individuals diagnosed as autistic in 2025 would meet the DSM-III criteria for infantile autism.
A revision of DSM-III, called DSM-III-R, was published only seven years later, effecting a significant broadening of diagnostic criteria for autism (APA, 1987). In DSM-III-R, the features of autism were described with 16 diagnostic criteria that were sorted into an 'autism triad' of three domains of impairment, in (i) social reciprocity, (ii) social communication, and (iii) repetitive behaviour. Crucially, autism was now operationalised as a polythetic, rather than monothetic disorder: to meet criteria, an individual did not have to demonstrate all listed features. Instead, they were required to meet a total of at least eight of the 16 diagnostic criteria, distributed across the three parts of the autism triad, with at least two in the social reciprocity domain. In addition, a subsidiary diagnosis of 'Pervasive Developmental Disorder – Not Otherwise Specified' (PDD-NOS) was described, encompassing those who showed some autistic features, but who did not meet the full criteria for autism. Compared to DSM-III, the autism diagnostic criteria of DSM-III-R encompassed a larger and more varied group of individuals, as was soon demonstrated by empirical studies, such as the DSM Field Trials (Rosen et al., 2021).
During the extensive collaborative process for agreeing on autism's next set of diagnostic criteria in DSM-IV (APA, 1994), there appear to have been tensions between those seeking to narrow the definition of autism and those pushing in the opposite direction (Silberman, 2015). The primary author of the DSM-IV autism diagnostic criteria, Fred Volkmar, had formed the view that DSM-III-R criteria were overly broad, and sought to redress this (Volkmar et al., 1992). Contrary to this was pressure from a group led by Lorna Wing to recognise in DSM-IV a new autistic subcategory, named 'Asperger's disorder'. Based on her clinical and research experience, and perhaps also her insights as the parent of an autistic child, she had understood that there were a group of autistic people who were excluded from a diagnosis under the DSM-III and DSM-III-R rubric. They tended to have reached early developmental milestones without significant delay and have a normal-range IQ and fluent speech. Such individuals are more evident in Hans Asperger's original paper than in Kanner's work. Wing had led the rediscovery in English-speaking circles of Asperger's paper and suggested that his name be used to describe this group of autistic people. The intention was that by making them entitled to a diagnosis, they would be more likely to receive the understanding and support that they needed. It should be noted that at this time, Asperger's complicity with the actions of the Nazi occupation of Vienna, including with its child euthanasia programme, was not well understood or widely known (Czech, 2018).
By the time DSM-IV criteria were being developed, the momentum towards the official recognition of Asperger's syndrome had become irresistible, even to those in charge of the project who sought to address what they saw as the overdiagnosis of autism in the wake of DSM-III-R (Rosen et al., 2021). Crucially, Wing and colleagues had already successfully lobbied for Asperger's syndrome to be included in the ICD-10 (1992), the World Health Organisation's diagnostic manual, widely used outside of the USA. The architects of DSM-IV placed value on there being concord between the diagnostic criteria used in the USA and internationally, and this was a key consideration in the inclusion of Asperger's disorder in DSM-IV (Rosen et al., 2021).
The tensions during the development of DSM-IV criteria between tightening autism's diagnostic criteria and extending them to include Asperger's syndrome were, with hindsight, a tussle between a narrow, categorical view of autism and a broader, dimensional one (Silberman, 2015). In diagnostic terms, Asperger's syndrome sits in a borderland between a clinical 'disorder' and subclinical high autistic traits. As such, the publication of DSM-IV, which sold over a million copies worldwide ("By The Book", 2013), was a crucial moment in the growing ascendancy of a dimensional conceptualisation of autism in mainstream research and practice.
The above-described and ongoing growth in diagnostic rates for autism took hold around the time that DSM-IV was published. Whilst DSM-5 (2013) later dropped the label of Asperger's disorder, subsuming various autistic subtypes listed in DSM-IV (childhood autism, Asperger's disorder, PDD-NOS) under the single category of 'autism spectrum disorder' (ASD), it did not preclude the diagnosis of those fitting an Asperger's profile. Nevertheless, DSM-5 was intended to stem rising rates of autism diagnosis and a perceived excessive broadening of the construct, in particular, in its elimination of PDD-NOS, which described people who met some but not all of the criteria for autism. Whilst technically DSM-5 did represent a narrowing of autism diagnostic criteria (Mandy et al., 2017), in practice this had no discernible effect on diagnostic rates, with rises continuing unchecked by its introduction in 2013 (e.g., see Figure 2).
Beyond considering changes to diagnostic criteria, there is empirical evidence that there has been a broadening of diagnostic criteria since the 1990s. First, the characteristics of those diagnosed have changed during this time, to include a greater diversity of presentations. In the DSM-III era, most people diagnosed with autism also had an intellectual disability. Post-DSM-IV, increasing numbers of people with normal-range IQ (i.e., fitting the Asperger's profile) came to be diagnosed (Keyes et al., 2012). As a result, in many high-income countries, such individuals now comprise the majority of autistic people. This is especially pronounced in the UK, where, as of 2018, around 90% of diagnosed autistic people do not have an intellectual disability (O’Nions et al., 2023). Second, there is some evidence that the level of autistic traits required for an autism diagnosis has fallen. A Swedish study using data collected between 1993 and 2002 found a five-fold increase in diagnoses in children, with no evidence for any corresponding increase in the level of autistic traits in the population (Lundström et al., 2015). Further, also in Sweden, it was observed that amongst children diagnosed with autism, the average level of autistic traits fell substantially between 2004 and 2014, which is consistent with the idea that the threshold for diagnosis had reduced during this time (Arvidsson et al., 2018). Third, there is some initial, suggestive evidence from Danish registry data that since 1994, the level of genetic susceptibility associated with an autism diagnosis has fallen (LaBianca et al., 2025).
It is helpful to make two points about the broadening of the diagnostic category of autism. First, in contrast to the example given for hypertension, the change to autism's diagnostic threshold was not a single, transparent, planned event. Rather, it arose over a period of several years, in a somewhat haphazard fashion, without being explicitly willed by a central authority. In fact, it could be argued that it happened despite the preferences of authorities, for example, Kanner and those within the American Psychiatry Association who sought to resist what they considered moves towards an over-inclusive diagnosis (Silberman, 2015). Much of the impetus towards expanding the autism category came, initially, from parents and clinicians, looking to ensure that those who might benefit from the diagnosis were more likely to receive it. More recently, as autistic people have gained more of a voice in how autism is understood, this has tended to provide an impetus towards further extension of the construct, for example, to include presentations more common in girls and women and people who do not pervasively show overt autistic characteristics due to having developed a capacity to mask (or 'camouflage') their autism (Bargiela et al., 2016).
A second point about the expansion of autism is that it has not resulted in a diagnosed population who have mild levels of clinical need. Even in countries such as the UK and USA, where some of the highest diagnostic rates are found, autistic people as a group experience very high levels of disability, alienation, and distress. In these countries, autistic young people, diagnosed under current conventions, have high rates of: mental health problems, social exclusion, peer victimisation, educational under-attainment, school exclusion, and self-harm (BLANCHARD et al., 2021; Brede et al., 2022; Roberts et al., 2025). They commonly struggle with the transition to adulthood, when they are at high risk of mental health problems, un- and under-employment, loneliness, poverty, poor mental and physical health and premature mortality (Lai et al., 2019; O’Nions et al., 2024; O’Nions et al., 2023). On this basis, the notion that the growth in autism prevalence rates indicates that the condition is currently overdiagnosed is wide of the mark. Those being diagnosed under broader criteria in countries such as the USA and UK show high levels of autistic traits (i.e., 'symptoms') and clinically significant levels of disability that are related to these.
What are the benefits of an autism diagnosis?
To summarise the argument so far, a key – likely the key – driver of the steep and ongoing rise in rates of autism diagnosis since the 1990s seen in industrialised nations such as the USA and UK has been a broadening of diagnostic criteria. I argue this was driven more by demand rather than supply: it was motivated by the needs of parents and autistic people, instead of being imposed by professional authorities. Based on a dimensional model of autism, the broadening of diagnostic criteria can be understood as a lowering of the diagnostic threshold for autism, such that lower levels of neurobiologically grounded autistic traits are now required for a diagnosis, compared to in the early 1990s and before. Whilst average levels of autistic traits are somewhat lower in the diagnosed population, levels of disability, alienation, and distress are high. I will now go on to explore one idea about why there has been a broadening of autism diagnostic criteria, and to that end, I will initially consider what function an autism diagnosis serves.
The empirical literature points towards two broad functions of an autism diagnosis. The first concerns identity and belonging. In this sense, a diagnosis of autism can be understood not only as a precursor to intervention, but as an intervention in and of itself. The qualitative literature on why adults seek an autism diagnosis emphasises the profound sense of alienation many autistic people feel growing up, especially after beginning formal education (Gellini & Marczak, 2024). A common metaphor used by autistic people to describe this is of being on 'the wrong planet', as in this statement from an autistic adult:
'The biggest memories I have is starting primary school and literally being on the playground and feeling like I was on an alien planet. I couldn't understand these children and I didn't understand how to interact with them, and everything they did was like a foreign language.' (from Atherton et al., 2022, p. 9)
Being a person with unrecognised high autistic traits in environments that are poorly suited to the individual's capacities and needs commonly has significant negative consequences for wellbeing and functioning (e.g., Brede et al., 2019). In this situation, many suffer high levels of distress, social alienation, bullying and academic under-attainment (Bargiela et al., 2016; Lai et al., 2019; Roberts et al., 2025). After such experiences, a subsequent autism diagnosis has been described as a 'not guilty verdict' (Gellini & Marczak, 2024; Punshon et al., 2009). It can enable the formation of a more positive personal identity by changing the individual's story about themselves, away from one that focuses on self-blame and a sense of personal failure, to one that explains past and current difficulties as arising from an undiagnosed and unsupported neurodevelopmental difference (Davies et al., 2024).
Further, receiving an autism diagnosis has social effects upon identity. These can be beneficial in contexts where there is an active community of autistic people and where positive attitudes to autism are present (Davies et al., 2024). For some, receiving an autism diagnosis brings with it a sense of belonging, which in turn can promote wellbeing and resilience. Amongst autistic young people (Cooper et al., 2023) and adults (Cooper et al., 2021), those who identify with autistic people as a group whilst holding positive views about autism report greater wellbeing and lower levels of mental health difficulties. There is a growing trend towards people self-identifying as autistic, without having received a diagnosis from a professional authority (Overton et al., 2024). Whilst this partly reflects difficulties accessing formal assessment, it also attests to the function of autism diagnosis as an intervention that can help reshape personal and social identity.
The second key function of an autism diagnosis is as a means of attaining support and accommodation, to improve wellbeing and functioning. The nature of the intervention that should follow an autism diagnosis has, in recent years, become contested. Traditionally, within the 'pathology model' described above, autism was assumed to be a disorder, with the implication that interventions should aim to reduce autistic impairments or even seek to 'cure' the condition. By contrast, it is an axiom of the neurodiversity model that autism is a form of difference, not disorder, that should be respected and valued. As such, within this paradigm, therapeutic attempts to reverse autistic impairments or to cure autism are seen, not only as liable to be ineffective, but also as immoral, being symptomatic of intolerance and stigma directed towards neurodivergence (Chapman & Botha, 2023).
Within the neurodiversity model, the disability, alienation, and distress so commonly associated with autism arise from the problem of being autistic in environments that are unaccommodating and, often, hostile. Accordingly, those within this paradigm emphasise the importance of working to enhance wellbeing in ways do not place all the onus on the autistic person to adapt to their environment; but which, rather, seek to make accommodations to provide a more enabling and comfortable ecology. This can take multiple forms and includes interventions to: reduce intolerance and stigma in peers (Zahir et al., 2024); modify the school environment (Bargiela et al., 2016); scaffold the transition to adulthood (Cooper et al., 2024); and support employment (Ashworth et al., 2024). Other ecological interventions that can follow an autism diagnosis include the adaptation of services, for example, those treating mental and physical health problems, to make them accessible and effective for people with high autistic traits (Brede et al., 2022). Within the neurodiversity paradigm, individualised interventions are aimed at flexibly and collaboratively addressing the needs of the autistic client; they should not be based on neurotypical assumptions about what a positive outcome looks like.
Shifts in the environment?
When autistic people seek an autism diagnosis, this is very commonly in response to high levels of disability, alienation, and distress, which arises due to a poor fit between them and their environment. Diagnosis is sought with the aim of redressing this, as it can help people make sense of their difficulties and suffering, with the potential to reduce self-blame and feelings of inadequacy and instead promote belonging and positive identity. Further, the diagnosis can inform the formulation of a person's difficulties and potentially open the door to support and accommodation: it can reduce distress and enhance function by improving person-environment fit.
The growing number of people seeking an autism diagnosis (and of parents seeking one for their children) can therefore be understood as an attempt to alleviate the challenges that are posed to people with high autistic traits by the environment. This raises the question of whether rates of autism diagnosis have risen continually since the 1990s, not due to changes in individual capacities, but rather because of shifts in what the environment affords people and what it demands of them. On this basis, in the remainder of this article, to understand why rates of autism have increased in many countries since the 1990s and to help address the question of 'what is autism, now?', I will explore the following proposal:
Important features of the environment have changed since the 1990s in ways that are especially challenging for people with neurobiologically grounded, genetically-influenced high autistic traits, thereby lowering the threshold at which autistic traits tend to be associated with clinically relevant levels of disability, alienation and distress.
This is an idea that has been proposed by the philosopher and leading scholar within the neurodiversity movement, Robert Chapman. In Empire of Normality, he writes that since Margaret Thatcher (the UK's first avowedly neoliberal Prime Minister) came to power 'the spectrum has continually widened as an ever-rising percentage of the population fall short of the social, communicative and sensory processing capabilities required by the new economy' (p.114; Chapman, 2023). The rest of this article will investigate and test this idea by reviewing literature from economics, sociology, and psychology. The aim is to take steps towards an empirical characterisation of specific shifts in the environment since the 1990s. My focus is mainly on changes to social demands, with the acknowledgement other autism-relevant shifts in the environment (e.g., in its sensory properties and demands for flexibility) warrant future investigation.
It is important to recognise that different modes of social behaviour should be assumed to be worse modes of social behaviour. Damian Milton (2012) has characterised the social and communication difficulties between autistic and non-autistic people as a 'double empathy problem': a mismatch between two different ways of relating. Accordingly, the social challenges experienced by autistic people arise not because of a deficit on their part but, rather, due to a relational misalignment in cross-neurotype interactions. In the upcoming discussion about the challenges for autistic people of meeting the escalating social demands of late modern societies, I frame this as arising from the double empathy problem, rather than as symptomatic of social 'deficits' on the part of those with high autistic traits.
The ascendancy of neoliberalism
From the 1980s onwards, there was a shift in economic conditions in many industrialised nations that has been labelled variously, including as a move from Fordism to Post-Fordism, the ascendancy of neoliberalism, the advent of advanced capitalism or the onset of late modernity. In the USA and UK, this transition is commonly linked to the governments of Ronald Reagan and Margaret Thatcher, respectively. The period since the 1980's has seen, in many advanced capitalist countries, a growth in inequality of both income and wealth, reversing a trend of declining inequality after the Second World War (Picketty, 2022). For example, in the USA, the income share of the top 10% of earners was 33% in 1970, and had risen to 50.5% by 2018 (Saez, 2018). It is estimated that of the growth in real incomes in the USA between 1993 and 2018, 48% went to the top 1% of earners (Saez, 2018). A similar, albeit less extreme, trend has occurred in the UK. A related phenomenon has been job polarisation, with the employment market becoming increasingly bifurcated into low- and high-income jobs, due to slower growth in the middle of the wage distribution (Edin et al., 2022). In this sense, competition for resources has intensified in neoliberal countries, with the winners taking an increasing share of the spoils.
'The new commandment of the late-modern society is the imperative to achieve' (Han, 2015)
In neoliberalism, competition is seen as both fundamental to human nature and as the best way to organise economic activity (Monbiot & Hutchison, 2024). It is viewed as both inevitable and as a productive force that should be untrammelled by regulation. Whilst this is an economic philosophy about how markets should be organised, the neoliberal valorisation of competition, and the economic conditions this fosters, have shaped society and the inner worlds of those who live within it. One formulation of this comes from the philosopher Byung-Chul Han, who has proposed that 'twenty-first century society is no longer a disciplinary society, but rather an achievement society' (Han, 2015). The disciplinary society is based around rules, restraints and compulsions imposed externally; whereas in the achievement society of late modernity, compulsion comes from within the subject, as an obligation towards positivity, self-improvement and accomplishment. Han asserts that the dictum of competitive striving that is central to the neoliberal economy has been widely internalised as a form of 'absolute competition', in which the individual 'succumbs to the destructive compulsion to outdo [themselves] over and over again'.
Beyond Han's philosophical analysis, there are empirical data to support that idea that the individualism and competitiveness required to participate in a neoliberal economy have, since the 1990s, increasingly permeated the values, attitudes, and beliefs of people living in advanced capitalist societies. Butler & Coward (2024), seeking to trace the impact of neoliberalism on mental health, argue that in late modern societies, young people's development occurs in 'differentiated and competitive social environments where opportunities and access to resources are unequally distributed'. Butler presents data to suggest that in this context, a cluster of extrinsic values have become more prominent and widespread in adolescents since the 1990s; namely, individualism, status-seeking, the drive for self-optimisation and status seeking (Butler, 2021; Butler & Coward, 2024).
Studies comparing different generations who have been assessed at a similar age for specific traits or values can help investigate the idea that neoliberal conditions since the 1990s have shaped the psychology of people in advanced capitalist societies. Research taking this approach has tended to show a shift during this time amongst young adults towards more individualistic, competitive, and materialistic ways of being. A meta-analysis of studies of perfectionism in college students between 1989 and 2016 in the USA, UK and Canada showed increases in this trait, overtime (Curran & Hill, 2019). The largest changes occurred in 'socially prescribed perfectionism', which concerns perceptions of exacting demands from others and the anticipation of harsh consequences if these are not met. In addition, 'other-oriented perfectionism' increased, indicating growing expectations put on others: not only do recent cohorts of young people expect more from themselves and feel greater externally-imposed demands, they also expect more from those around them (Curran & Hill, 2019).
In the USA, individualism and extrinsic values, such as increasing importance placed on money, fame, and image, have grown in prominence amongst young adults since the 1990s (Twenge et al., 2012). Simultaneously, intrinsic values concerning the importance of affiliation, community, and self-acceptance have declined (Twenge et al., 2012). In a similar time frame, self-reported narcissism, which is associated with greater competitiveness and lower connection to others, has risen amongst US college students (Twenge & Foster, 2010). Consistent with this, in a similar population, 'empathic concern' (i.e., sympathy for the misfortune of others) has fallen since the 1980s (Konrath et al., 2011).
The hyper-social age
In an increasingly competitive and individualistic culture, what capacities are required to succeed? In this section, I focus on one particular set of abilities that concern social relating and communication. My argument is that since the 1990s, for children and adults in advanced capitalist countries, there has been an escalating expectation of sociability, with the ever-growing requirement that individuals develop and deploy a specific set of social and communication skills. These rising social demands have particularly taxed those with high, neurobiologically grounded, autistic traits, thereby lowering the threshold at which such traits engender disability, alienation, and distress due to poor person-environment fit.
Two structural changes in the nature of work in the neoliberal era have directly intensified the requirements for sociability and social-communication performance in people's daily lives. First, the workplace has become increasingly computerised so that ever-more tasks previously done by people have been taken over by computers. On the whole, this has made working life less routinised and predictable (Deming, 2017). This is because computers are adept at performing routine, rule-based activities, but cannot currently outdo humans in flexible, open-ended activities, including those centred on social interaction. Computerisation of the workplace tends to push workers towards more team-based settings, where communication, social skills, and flexibility are at a premium (Autor et al., 2003). Autor & Price (2013) found that, when considering different types of worker tasks in the US economy, it was non-routine interpersonal tasks that grew the most in frequency between 1960 and 2010, whilst the requirement for non-routine tasks declined.
Second, is the ongoing growth in the proportion of workers in the service sector, with a corresponding decline in those working in agricultural and industrial roles. This includes a growing proportion of people working in jobs where social interaction and the management of others' feelings are a central work task. When considering high-skilled cognitive occupations in the USA between 2000 at 2012, Deming (2017) observed that the fastest-growing roles in terms of their share of the overall job market (teachers, managers, nurses, therapists) all involved significant social interaction. This trend is not limited only to professional jobs requiring high levels of education. Between 1980 and 2012, jobs with significant social skill demands grew by 11.8% as a share of all jobs in the US economy (Deming, 2017). Aghion and colleagues (2023) examined trends in the UK between 2004 and 2019 in occupations that did not require a college education. They found that jobs which had minimal social requirements declined relative to jobs placing high importance on social skills, which markedly increased.
Data on which personal characteristics are associated with high wages and with wage growth further illustrate that importance of sociability and social skills at work has risen significantly since the 1990s. In the USA, social skills predict higher wages, and this effect has grown over time: the economic return on social skills was larger in the mid-2000s compared to the 1980s and 1990s (Deming, 2017). This was replicated in a sample of Swedish men whose social and cognitive traits had been directly measured when conscripted for national service (Edin et al., 2022). In this analysis, the most striking growth in the importance of social skills for wages occurred during the 1990s. Another notable finding was that growth in the importance of cognitive skills in predicting wages appears to have ceased to increase during the 2000s, suggesting the ever-growing importance in the labour market of social skills (Deming, 2017; Edin, 2022).
The work of sociologist Arlie Russell Hochschild provides a powerful analysis of the subjective experience of this type of interpersonal work, including the demands it places on the worker. Based on her ethnographic work with flight attendants and bill collectors, in The Managed Heart: Commercialization of Human Feeling, Hochschild (1983) derived the concept of 'emotional labour', whereby workers are required to suppress or mould their true feelings, to enable the performance of an outward countenance that serves to produce the proper state of mind and feeling in clients. Emotional labour is a resource that is sold by the worker and, also, a work-place obligation. Hochschild points out that it involves, via training and performance management, the control by employers of their employees' emotions and social behaviour.
Emotional labour is not just the preserve of airline stewardesses and bill collectors, of course, as the management of other people's feelings is part of most jobs. As has been argued above, it is ever-more integral to much work in advanced capitalist societies. Emotional labour draws upon a range of capacities, including: sensing (often unstated) rules about social norms of the workplace; regulating authentic emotion; using verbal and non-verbal behaviour to strategically perform certain feeling states; reading the verbal and non-verbal communications of clients; and being able to respond flexibly and spontaneously to the unpredictable challenges presented by clients' emotional states. Whilst many autistic people have successful and satisfying careers in jobs that have a large social component; nevertheless, due to the double empathy problem, these are all acts that tend to be harder and more effortful for people with high autistic traits.
Hyper-sociality in childhood
To what extent have the occupational demands of modern economies infiltrated daily life, beyond the workplace? And have these intensifying requirements for sociability and a certain type of social skill in the adult workforce affected childhood, when most autism diagnoses are made? To explore these questions, I will consider changes to education in the USA and UK, since the 1990s, with a particular focus on the growing importance that has been placed on fostering and monitoring the development of 'social and emotional learning'.
The transition to late capitalist society is associated with parents having fewer offspring than in earlier generations and investing more intensively in the development of each of their children (Morita, 2018). This is particularly characteristic of parents who have attained high-wealth and status (Butler, 2021). These shifts in fertility and childrearing can be understood as a strategy whereby parents intensively focus resources on developing each child's embodied capital in the hope this will enable that child to thrive in a highly competitive, skills-based adult world (Butler, 2021). Embodied capital refers to the knowledge and personal capacities that an individual attains. As outlined above, the nature of the embodied capital valued in the workforce has shifted since the 1990s, with an increasing premium placed on sociability and social skills, in addition to cognitive abilities. Education systems in late capitalist societies have responded to this, by placing greater emphasis on social development in addition to the traditional educational outcome of academic attainment.
Social and emotional learning (SEL) is an approach to education that aims to foster the development of a range of 'non-cognitive' capacities, outside of core academic outcomes, including social awareness, self-management, responsible decision-making, self-awareness, and relationship skills (Elias et al., 1997). Drawing on theoretical and applied work of psychologists and teachers in the New Haven area in the USA, SEL was formalised as a coherent, defined educational method in the mid 1990s, with the foundation of the 'Collaborative to Advance Social and Emotional Learning' (CASEL, since renamed the 'Collaborative for Academic, Social, and Emotional Learning'). CASEL was founded in 1994, a year before the publication of Goleman's (1995) internationally best-selling and influential book 'Emotional Intelligence: Why it can matter more than IQ'. It is notable that the SEL movement emerged at exactly the same time that non-cognitive skills were becoming especially important for labour market success; and that a key, explicit goal of SEL is to prepare students for the workplace.
Since the 1990's, SEL has rapidly grown in prominence and become a fundamental part of educational practice in late capitalist countries, including the USA and UK (García & Weiss, 2016). Organisations promoting SEL have proliferated internationally, and the monitoring and promotion of non-cognitive skills in education is widely endorsed by lawmakers and policy makers. The UNESCO Incheon Declaration for Education 2030 declares that 'Relevant learning outcomes must be well defined in cognitive and non-cognitive domains, and continually assessed as an integral part of the teaching and learning process. Quality education includes the development of those skills, values, attitudes and knowledge that enable citizens to lead healthy and fulfilled lives, make informed decisions and respond to local and global challenges.' A national implementation survey by CASEL in 2024 found 83% of principals in US public schools reported using a SEL curriculum, up from 76% in 2022. In a survey of UK primary schools, 46% reported that SEL was their top priority, with a further 49% describing it as important alongside other priorities (Wigglesworth et al., 2021).
The rise of SEL since the 1990s marks a wider trend, which is the growing importance given to the social attainment of children in late modern societies. School environments are increasingly demanding of the social capacities of their pupils. Pedagogic methods have shifted away from teacher-centred, rote-learning approaches towards student-centred teaching that emphasises collaboration, back-and-forth interaction, presentations and group work. In this context, with the wide-spread acceptance that non-cognitive skills are a key educational outcome, the social behaviour of each child is increasingly monitored and benchmarked against normative standards. One example of this is the Organisation for Economic Co-operation and Development (OECD) initiative to promote SEL, which includes its international Survey on Social an Emotional Skills (SSES), launched in 2019 to assess 'the creativity, curiosity, empathy, co-operation and other social and emotional skills of 10- and 15-year-old students in nine cities from different regions of the world' (O.E.C.D., 2023). The OECD promotes universal monitoring of SEL, noting with disapproval that in their sample 'the social and emotional skills of one in three 15-year-old students and one in four 10-year-old students are not assessed in school'.
My aim is not to characterise the rise of SEL and the increasing focus on non-cognitive outcomes in education as an inherently negative development. Clearly, there is a range of benefits to supporting the social and emotional development of young people in school, as attested by empirical studies (Durlak et al., 2011). But I do highlight two impacts on people with high autistic traits and on rates of autism diagnosis. First, by placing ever-greater demands on specific, narrowly-defined social capacities in school, it is likely that an ever-larger group of people who struggle to meet these demands is created. In relation to pupils with high autistic traits, this effectively lowers the threshold at which disability and distress are experienced. There is little evidence that the definitions of social skills within SEL programmes and assessment accommodate autistic styles of interaction and communication (O.E.C.D., 2023). Second, the monitoring and benchmarking of pupils' social performance, in combination with the importance placed on it, means that those who struggle to meet conventional norms in this area are especially likely to become the subject of concern. The application of standardised testing of social capacities likely narrows the range of social styles that are considered to represent successful, healthy development in a way that is unhelpful for many neurodivergent people.
Conclusion
The substantial and ongoing rise in rates of autism diagnosis in many high-income countries, which started in the 1990s, has led some to talk of an 'autism epidemic' and others to warn that overdiagnosis is occurring. In this article, I propose a different explanation. Rising autism rates reflect a broadening of diagnostic criteria to encompass a wider range of autistic presentations and lower levels of autistic traits. However, this is not the same as overdiagnosis: those who have been encompassed by the broadening criteria still have high levels of autistic traits, and these are commonly associated with significant disability, alienation and distress. The disability of people with high autistic traits arises from living in a world built largely by and for non-autistic people, which commonly causes a misfit between them and their environment. On this basis, I propose that broadening of autism's diagnostic criteria has been partly driven by changes in the environment since the 1990s, which have posed escalating challenges for people with high autistic traits.
When seeking to characterise the nature of these environmental changes, I have argued for an escalation of social demands placed on people across the lifespan in late capitalist countries (Chapman, 2023). Since the 1990s, neoliberal societies have become increasingly individualistic and competitive; and success in this competitive milieu has become ever-more dependent on the performance of a set of neurotypical social and communication skills. This has created an expanding group of people who, due to their autistic traits, experience disability, alienation, and distress. For many of these people, an autism diagnosis, and the identity that can come with it, is a means of making sense of and coping with the challenges that commonly arise from having autistic characteristics in a competitive, hyper-social environment. Action is required to make environments (e.g., at school and in the workplace) less narrow in their demands on the individual, to allow a wider range of people to thrive.