1. INTRODUCTION
Research from the US, European and some Asian countries identified a relatively low vaccination rate for the first generation of COVID-19 vaccines after their release (Sallam, 2021; Fridman et al., 2021; Troiano & Nardi, 2021). To end the pandemic, greater acceptance of the COVID-19 vaccine is essential. To identify predictors of vaccine hesitancy and willingness to get vaccinated will help public health campaigns become more effective. In the present study, we add to the exploding literature that tries to explain COVID-19 vaccine hesitancy by exploiting a large survey data set that comprises more than 1.5 million respondents on Facebook from 23 countries : the United States; 10 countries in Asia (Bangladesh, India, Indonesia, Japan, Malaysia, Pakistan, Philippines, Thailand, Turkey, Vietnam), two in Africa (Egypt, Nigeria), six in Europe (France, Germany, Italy, Poland, Romania, United Kingdom) and four in Latin America (Argentina, Brazil, Colombia, Mexico).
Vaccine hesitancy is a highly complex issue. A literature review on acceptance of the influenza vaccine came up with more than 70 potentially influential factors (Schmid et al., 2017). Other systematic reviews and meta-analysis drew similar dense pictures for other vaccines (Sheeran et al., 2014; Kohlhammer et al., 2007; Brewer et al., 2007; Larson et al., 2014) Various conceptual models exist. Among the most prominent is the 3-C or WHO model of vaccine hesitancy which identifies three core factors: confidence in the form of trust in the vaccine and the provider; complacency about the health risk posed by a virus to self and others; and convenience or easy access to vaccination (MacDonald, 2015). Other behavioral theories have been applied to identify perceptions and attitudes towards vaccines too -- for example, the health belief model (Coe et al., 2012), the theory of planned behavior (Britt et al., 2014), and models from moral psychology (Amin et al., 2017; Rutjens et al., 2018). All of these models try to capture the intricacy and variability of vaccine hesitancy and stress the complexity of vaccine hesitancy and beliefs which is further multiplied by context-specifics.
In this study, we work with an existing third-party data that comes from an omnibus survey on COVID-19 related beliefs, attitudes and behaviors. Attitudes on vaccination were only a side focus of the survey, so we have to concentrate on three types of variables which, however, have been shown to be pertinent for the decision to get vaccinated. The first cluster comprised risk perceptions with regards to the virus. Prior research has established that risk perceptions at the individual level (Betsch et al., 2015; Sheeran et al., 2014; Brewer et al., 2007 for review; WHO, 2017) and messages that emphasize the threat posed by a disease (Horne et al., 2015) played an important role in shaping vaccination intent. In the context of COVID-19, studies have demonstrated the impact of health-related beliefs too. Perceptions of COVID-19-related risks to individual and community health, perceived self-efficacy to avoid infection, and perceived health status all partly explained vaccine intent specific to COVID-19 vaccine (Kelly et al., 2021; Robertson et al., 2021; Mills et al., 2020). Moreover, accurate information about risks associated with the vaccine as well as acknowledgment of concerns raised by people reduced some of the confusion created by disinformation and increase intentions to get vaccinated (Mills et al., 2020).
The second cluster focuses trust in health authorities and is closely related to accurate risk perceptions. In 2020, the pandemic was labeled an infodemic and misinformation has been rampant, particular on social media (Biswas et al., 2021; Hao & Basu, 2020; Viswanath et al., 2021; Rivas et al., 2021). As such, factual information sources of high quality have been essential for a proper understanding of the virus and the strategies to contain it (Browne et al., 2015; Dror et al., 2020; Lazarus et al., 2021). However, for people to select and process this information, it is necessary that they trust the communicator. Prior studies clearly demonstrated that mutual trust between communities and public health sectors is key for vaccine acceptance (Attwell et al., 2018; Palamenghi et al., 2020; Verger & Dubé, 2020; Yaqub et al., 2014). Relatedly, higher trust in government (Lazarus et al., 2021) and in science (Plohl & Musil, 2021) were also associated with increased acceptance of the COVID-19 vaccine, with health workers reported as particularly trusted sources for vaccine guidance (Arce et al., 2021). Consequently, mistrust in healthcare and government and a lack of confidence in scientists went hand in hand with lower acceptance of vaccination (Biswas et al., 2021; Murphy et al., 2021; Viswanath et al., 2021).
Our third cluster comprises demographic core variables, namely gender, age and education. A recent review suggested that lower levels of education seem to be associated with lower COVID-19 vaccine acceptance in some countries, but their results were mixed for higher level of education (Troiano & Nardi, 2021). The same review highlighted age as a pertinent factor with the younger demographic showing more resistance. However, again results are mixed, with another study observing the opposite trend with the middle-aged group showing reduced willingness (@palamenghi2020a). More consistently, various surveys of people from the US (Kelly et al., 2021, Malik et al., 2020) and from Europe (Neumann-Böhme et al., 2020) revealed gender based-differences with women being less likely than men to get vaccinated.
The inconsistency with regards to demographics can be read as indications for a context dependency of intent to get vaccinated against COVID-19. Indeed, existing research suggests that vaccine acceptance has not only been influenced by individual-level factors, but that characteristics on the country-level matter too. For example, significantly lower acceptance rates for COVID-19 vaccines were found in countries with a history of vaccine mistrust (of Global Health Innovation, 2021; Fridman et al., 2021; Kelly et al., 2021; Malik et al., 2020). Moreover, pre-pandemic vaccination practices within a country (e.g., against the H1N1-virus) predicted COVID-19 vaccine acceptance in ways that reflect cultural and political disparities (Chor et al., 2011).
Altogether, these clusters were determined to be important possible contributors to vaccine hesitancy, therefore we examined how COVID-19 vaccine acceptance systematically varies with risk perceptions, trust in health authorities and demographics. We also explored the extent to which country-specifics override potential individual-level effects." By including various countries in Africa, Asia and Latin America we partly address their underrepresentation in prior comparative work around COVID-19 (e.g., Kelly et al., 2021; Murphy et al., 2021; Neumann-Böhme et al., 2020).
2. Method
2.1 Data source
We used data collected from a global survey of Facebook users for our study. Our analysis is therefore based on a prechosen set of variables and measures. The survey was an omnibus-survey themed around COVID-19 beliefs, behaviors, and norms. The survey was conducted by the Massachusetts Institute of Technology in collaboration with Facebook, with input from researchers at Johns Hopkins University, the World Health Organization, and the Global Outbreak Alert and Response Network. It was implemented as rolling cross-sections with 19 bi-weekly waves (Collis et al., 2022). Although several measures were taken to minimize the representation error, we do not treat the data as being representative in the narrower sense for the country population. Full information about the data collection is available at https://covidsurvey.mit.edu.
2.2. Measures
The survey measured intent to get vaccinated by asking respondents whether they "would choose to get vaccinated" (in the earlier waves: "if a vaccine became available"). Answering options were "yes", "no" and "don't know". In later waves, respondents could report their actual vaccination. We grouped those who got vaccinated and those who were willing to get vaccinated into one group, because vaccination was not mandatory in any of the countries at the point in time. Hence, being vaccinated can be equated with intend to vaccinate a day before vaccination.
Four types of COVID-19-related risk perceptions were assessed in the survey. Control beliefs were measured by asking respondent to give their agreement with the statement "I have control over whether I will get COVID-19" on a 5-point Likert-type scale. Threat to the community was measured by asking respondents how dangerous they thought the COVID-19 risk is to their community – with answering options ranging from "not at all dangerous" to "extremely dangerous" on a 5-point scale. Individual risk of infection was assessed by asking respondents how likely it is that someone of their age became sick from COVID-19 in their community - with answering options ranging from "not at all likely" to "extremely likely" on a 5-point scale. Finally, to measure perceived severity respondents were asked how serious it would be if they became infected with COVID-19 with answering options being "not at all serious", "somewhat serious", "very serious". Finally, and unrelated to COVID-19, respondents were asked in one item to rate their own health in general on a five-point scale ranging from "poor" to "excellent".
Trust in health authorities was measured as part of a larger section where respondents were asked how much they trusted sources when it comes to COVID-19 news and information. Answering options included "do not trust", "somewhat trust", and "trust". We averaged item scores for the following sources: "local health workers, clinics, and community organizations", "scientists, doctors, and health experts", "World Health Organization (WHO)".
The following socio-demographics were part of the survey. Gender was measured offering "male", "female" and a third non-binary "other"-option (the "other" option was not available in Nigeria, Bangladesh and India). Age was measured in decades ("under 20", "21-30", "31-40", etc.) Education asked for the highest level of education, offering five classes of degrees ("less than primary school", "primary school", "secondary school", "college/university", "graduate school").
2.3. Sample
For this study, we pooled data from waves 9 (November 2020) to wave 19 (March 2021) and selected from only those who completed our scales of interest leaving over 60,000 responses. At the time of wave 9, the first vaccines were approved, wave 19 was the last wave of the project. Pooling our data in this way implies that we are able to speak about predicted respondents' intent to vaccinate in the first months after the approval of the vaccine. While the vaccines were not globally available at this point in time, vaccination had become, at least in principle, a behavioral option for the near future.
We included respondents from all 23 countries. In the final data set, respondents were well distributed over the countries, ranging from a minimal of n=2,032 for India to n= 3,266 for Germany.
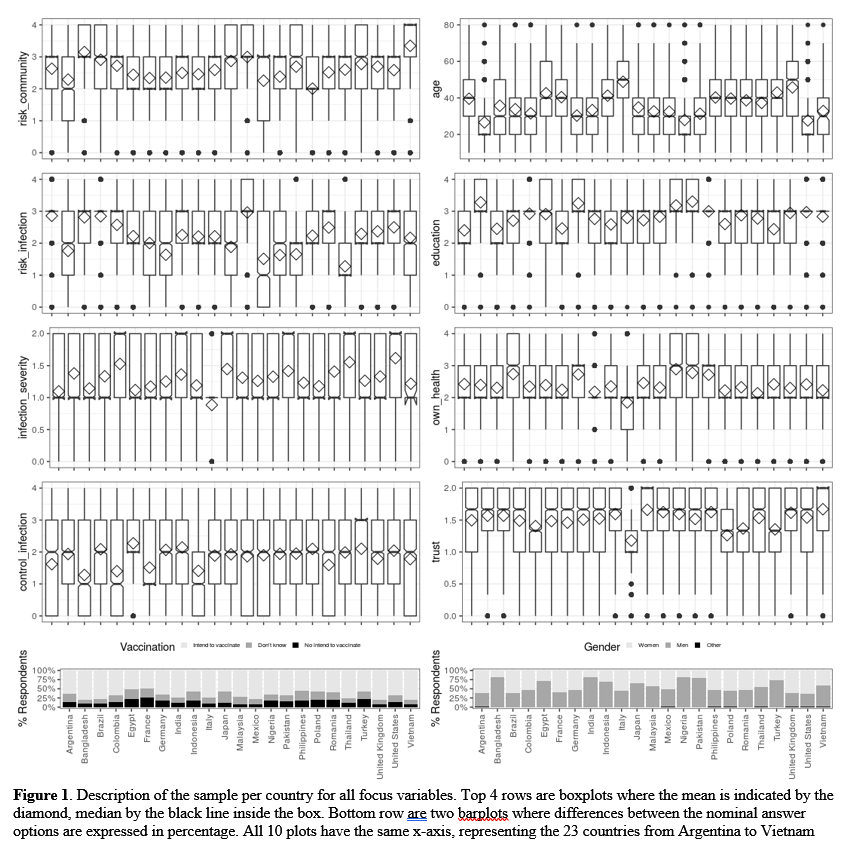
All respondents with valid data on focus variables were included in the analysis. Our remaining sample (N = 63,042) showed a well-balanced heterogeneity with regards to socio-demographics : (45%) were female, (54%) male, and (1%) identified as "other." 3.4% were less than 20 years old, 23.2% were between 20 and 29 years old, 23.4% were between 30 and 39 years old, 19.5% were 40-49, 16.3% were 50-59, 10.2% were 60-69, 3.5% were 70-79, and 0.5% were older than 80 years. Less than 0.5% indicated that they had not completed primary school; 3.5% had completed primary school, 29% secondary school, 48.3% college/university, and 18.6% graduate school. See figure 1 for a breakdown by country (see figure 1 for a distribution of the demographics and predictor variables by country).
2.4. Analysis
We used the R software environment to run multinomial regressions. Our categorical outcome was intent to get vaccinated and we used those who were willing to get vaccinated as reference group. Our predictors were age, gender (female as reference group), education, own health, control of infection, risk for the community, risk of infection, severity of infection, and trust in health authorities. All variables except gender were z-scored. For our main analysis, we pooled respondents from all countries and all waves into one global data set (n=63,042). For an additional explorative step, we re-ran the analysis per country pooled over all waves. We had to remove identification with a non-binary gender as a category for gender since it was not assessed in all countries.
3. Results
Before presenting the results of our regressions, the mere numbers of vaccine acceptance is notable. Of the 63,042 respondents from 23 countries in our pooled sample, 66.3% reported intending to be vaccinated or were already vaccinated. 19.1% indicated being indecisive and 14.6% reported not intending to be vaccinated (see Figure 1). Since the first generation of vaccines has been considered the central tool to contain the spread the virus and curb causalities in the months, these figures show the challenges for health authorities.
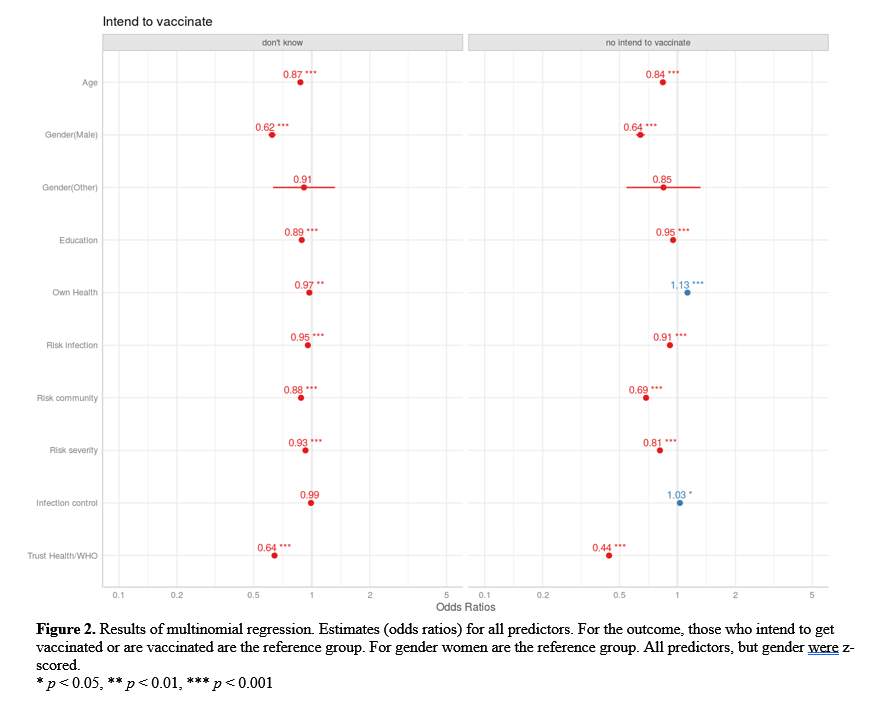
Figure 2 shows the results of the multinomial regression for the pooled global sample. First, we contrasted those who were willing to get vaccinated (or were vaccinated) with those who were not. We found that respondents of higher age, higher education, male gender, a higher perceived threat for the community, a higher perceived risk of infection, a higher perceived severity of infection, and higher trust in health authorities were more likely to be willing to get vaccinated. On the other hand, those who rated their own health as better and those who felt more in control over about their chances of getting infected were less likely to be willing to get vaccinated.
All of the aforementioned effects were statistically significant. Identifying with the non-binary gender option also increased the likelihood of intending to get vaccinated, yet not significant. Since we z-scored all predictors, the odds ratios represent a change of the odds of not getting vaccinated over getting vaccinated after a change of one standard deviation of the predictor. While we do not want to overinterpret small differences between the predictors, trust in health authorities seemed to be a particularly potent factor in our model.
When we contrasted those who were willing to get vaccinated (or were vaccinated) with those who were undecided, we found the same pattern with regards to effect direction and significance and the effect size of trust. Only respondents who had a better rating of their own health were also less likely to be undecided about their intent to get vaccinated. Moreover, the effect for control of infection were no longer statistically significant.
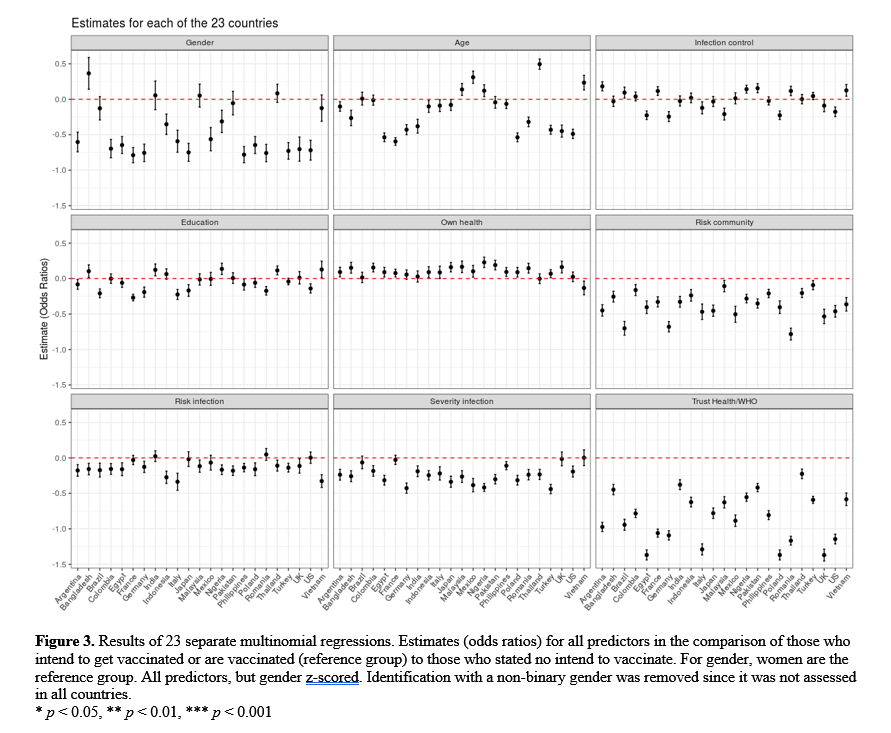
Figure 3 shows the results for 23 multinomial regression models, run separately for each country in our sample and focusing on the contrast "between the intend to vaccinate" group and the "no intend to vaccinate group". The first finding is that the effect direction for most psychological variables is rather similar for the different countries. Threat to community and trust in health authorities reduced the likelihood to be un_*willing to get vaccinated in all 23 countries. Risk of individual infection and perceived severity reduced unwillingness to get vaccinated, perception of own health increased the likelihood of unwillingness in all but four to five countries. Having said this, the variance of the odds ratios was larger for threat to community and trust in health authorities than for the other variables. Again, the change in odds ratio was the largest for a change in one standard deviation of trust. The only predictor that did not produce a conclusive pattern and varied strongly with country was perceived control over infection
The effects of socio-demographics showed slight variance over countries. In various, but not all Asian countries in our sample, the gender effect was non-significant, in Bangladesh even significantly reversed. Age was non-significant or even increased unwillingness in more than a handful of countries. Education did not yield a conclusive effect pattern and varied strongly with country.
4 Discussion
4.1. Vaccine intention
The current study investigated three clusters of pertinent variables (i.e., role of risk perceptions, trust in health authorities, and socio-demographic factors), in predicting future COVID-19 vaccination intentions across 23 countries. The importance of exploring predictors of COVID-19 vaccination hesitancy was supported by the relatively low rates of vaccine hesitancy in the months following the announcement of the vaccine (see also, Kelly et al., 2021; Lazarus et al., 2021; Robertson et al., 2021). Overall, findings from the global pooled sample and individual country models reproduce and extend prior research (e.g., Palamenghi et al., 2020) supporting the importance of these clusters in examining vaccine hesitancy as well as the robustness of these effects in a large, multi-country sample that included many Non-Western countries. Importantly, results were also consistent with models of vaccine hesitancy and beliefs (e.g., MacDonald, 2015).
For the first cluster, risk perceptions, a higher perceived threat for the community, a higher perceived risk of infection, and a higher perceived severity of infection were all associated with willingness to get vaccinated (see also Kelly et al., 2021; Robertson et al., 2021; Mills et al., 2020). Interestingly, those who rated their own health as better as well as those who felt they had higher perceived control over becoming infected were more likely to be unwilling to get vaccinated. While own health had the same effect in almost all countries, the effect of control varied strongly. This seems intuitive since locus of control will likely depend on local infection rates and prevention behavior in the community. This also mirrors findings regarding protective behavior more general (e.g., Mækelæ et al., 2020, Mækelæ et al., 2021).
For the second cluster, social trust in health authorities, those with higher trust in health authorities were more likely to get vaccinated or intend to be vaccinated. This strong effect of trust suggests the importance of trust in local and global health experts, including the WHO, and scientists in the increased likelihood of intending to get vaccinated. This supports past research highlighting the key nature of trust in those communicating health-related information as well the pivotal role of health authorities in supporting vaccination efforts (Attwell et al., 2018; Lazarus et al., 2021; Palamenghi et al., 2020; Plohl & Musil, 2021; Verger & Dubé, 2020; Yaqub et al., 2014).
Third, with regards to the socio-demographic cluster, we found that among our more than 60,000 respondents, men and older individuals were more likely to intend to and get vaccinated. In addition, those who had higher levels of education were also more likely to be willing to get vaccinated. However, the effects of socio-demographic factors varied more strongly between countries than trust and risk perceptions. This mixed finding is also in line with prior research (Murphy et al., 2021; Neumann-Böhme et al., 2020; Palamenghi et al., 2020; Plohl & Musil, 2021).
Future research could extend our findings by monitoring whether the influence of our core factors changed over time. In this initial phase, trust may have been more important since side effects were largely unknown and only few peers may have been vaccinated. Moreover, what the substantial reasons for the variability in effects of socio-demographics were and locus of control were.
4.2. Implications for Health Communication Practitioners
Understanding what factors influence vaccine hesitancy can provide helpful information for the ongoing public health planning to increase vaccination rates. In this regard, our findings provide a backdrop against which practitioners of health communication could evaluate campaigning in the first months after the announcement of the first generation of COVID-19 vaccines to learn. First, in that specific period in time, the population segments that were the best candidates for targeted communication across the globe (or at least in the 23 countries included in this sample) were younger, female, and-or less educated people. Second, nevertheless, global campaigns should be sensitive to national idiosyncrasies. Third, campaigns should target the health-related beliefs of their audiences: campaigns should highlight the risk of infection for individuals and the community and limited control that respondents have over getting infected or seriously sick. This is likely to work across national contexts. Third, our study highlights a serious challenge: Those who were less likely to get vaccinated also tended to have lower trust in health authorities. In other words, those who could potentially benefit the most from health information, were the least to attend to it. This finding highlights the detrimental effects of the erosion of institutional trust and the need for health communicators to constantly build institutional trust, also outside the pandemic. Fourth, communication should address the uncertainty pertinent in a pandemic (McGuire et al., 2020; Pearce, 2020; Piltch-Loeb & Abramson, 2020; Porzsolt et al., 2021; Rafkin et al., 2021; van der Bles et al., 2019). Being transparent about what is not yet known and that recommendations can change, foster trust. Omitting uncertainties decrease trust.
4.3. Limitations
This study worked with secondary data and is, therefore, limited in two ways. First, we had to rely on a prechosen set of variables and measures. In the Facebook omnibus survey, questions did not specifically focus on vaccine hesitancy and did not include all constructs from one of the common models like the 3-C-model (MacDonald, 2015). While crucial predictors of vaccine hesitancy are missing, we believe that this does not question the validity of our measures since we cannot think of any omitted variable bias. Moreover, while our measures have high face-validity, measures with known psychometric properties and established measurement equivalence across cultural contexts would have strongly strengthened our results.
Second, our data is not representative for the populations of the countries. Not only do Facebook users tend to differ from the general population. Access and usage of Facebook and participation in the survey may systematically vary with country (see figure 1, age and gender distribution).
While these limitations may account for the inconsistencies with regards to socio-demographics, the consistent effect of trust, threat to community, and severity of infection still hold. Therefore, we believe that our analysis provides another important piece for the large puzzle to understand skepticism against one of the main measures to curb the major health crisis of the last 100 years.
ACKNOWLEDGEMENTS
We would like to thank Facebook and Massachusetts Institute of Technology for giving us access to survey data and Martin Riegels for helping with the literature review.
REVIEW COMMENTS
R1: Marvin Starominski-Uehara
The topic of the paper is relevant and its results original. However, there are fundamental points to be addressed, particularly in regards to research question and hypotheses as far as disclosed limitations are concerned. I commend authors for this effort and WPRN for creating a platform that fosters mutual support and creativity among researchers.
R2: Francesca Ervas
The paper provides an interesting and timely contribution on vaccine hesitancy in pandemic times, highlighting its connection to both trust in health authorities and socio-demographic features. The results of the study suggest – in line with previous literature on the topic – that trust in health authorities and socio-demographic features, i.e., being men and older individuals with higher education and a higher perceived threat for both themselves and the community.
More words could be spent on the description and the discussion of the models of vaccine hesitancy and beliefs (e.g., MacDonald, 2015). The point is relevant to better understand vaccine hesitancy in the case of Covid-19 as a multilayered and context specific, i.e., varying across place, time, and specific vaccines. We might think that the results of the study can be explained by cultural aspects connected to the understanding of vaccination as a collective phenomenon: indeed, how people construct their beliefs on vaccination is usually biased by their beliefs on social groups and movements in their own culture.
Author's Response
We thank both reviewers for their very constructive feedback and suggestions for further research. We have addressed most of the suggestions. See the response letter for more information about some of the suggested edits.